
For patients and laymen
Overview
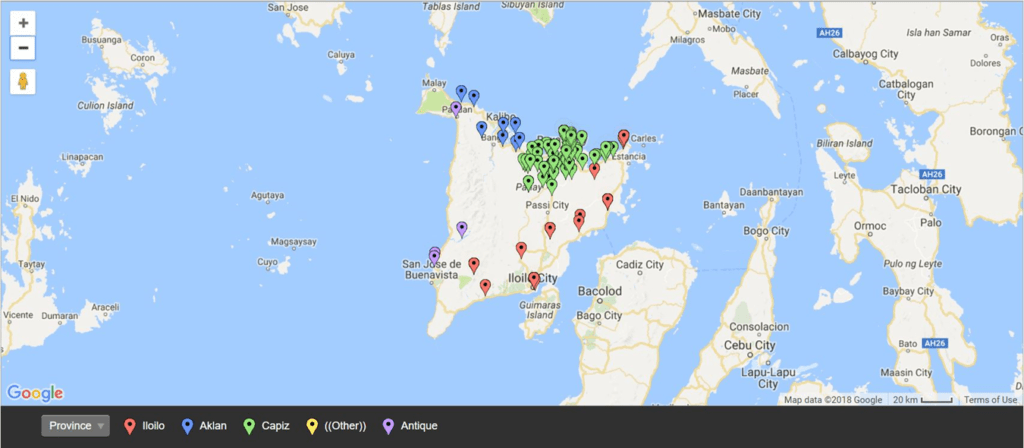
X-linked dystonia parkinsonism (XDP, DYT3) is an adult-onset sex-linked neurodegenerative movement disorder with features of both dystonia and parkinsonism. It is endemic to the Panay Island in the Philippines and cases described elsewhere are all linked to Filipino ancestry. The national prevalence in the Philippines (in 2011) is 0.31/100,000.
History
Sex-linked recessive dystonia parkinsonism (XDP) is a movement disorder first reported in 1975 on patients from the island of Panay, Philippines. Dr George H. Viterbo, of Roxas City, Capiz (a province of Panay) referred to the neurology section of the Philippine General Hospital in the early 1970s, five of the six cases of what then was rare ‘dystonia musculorum deformans’. This initiated an epidemiologic survey, which resulted in the first paper published in 1976. In the original paper, Lee et al. described 28 adult male cases with torsion dystonia, from 25 families. There was no male to male transmission hence, the inference of sex-linked recessive transmission. Some of the patients were noted to have parkinsonian features and some had relatives with parkinsonism.
Clinical Manifestations
Presentation and Course
Even before patients notice, x-linked dystonia parkinsonism may already affect balance, gait, eye movement, and sense of smell. The true start is likely mild stiffness and slowness, often unnoticed for a long time.
For most people, consult with a physician and diagnosis is prompted by dystonia, sustained or repetitive muscle contractions which cannot be controlled. It may start in a limb, the neck, jaw, or as excessive eye blinking. It spreads over time in almost case, often to many parts of the body within 5 years.
Over time, an average of 7 to 10 years from time of diagnosis, the dystonia starts to fade away, and what is left are the symptoms similar to Parkinson’s disease: stiffness, slowness, tremor, gait and speech problems.
The disease is linked to the x-chromosome, of which males have one, and females have two. Females with one abnormal copy of the gene may only have mild or little symptoms, but those with two can have the same as in males.
Diagnosis
X-linked dystonia-parkinsonism (XDP) is diagnosed through a combination of family history, neurological exam, and genetic testing.
Genetic testing is available at the Philippine General Hospital (PGH) and Makati Medical Center (MMC).
Management
In the early stages, XDP is treated only with medication. A number of possible medications may be given, depending on the patient. One commonly given is zolpidem. In the early stages it can greatly reduce or eliminate symptoms. As the disease progresses however, increasingly larger doses may be required.
For specific dystonias which do not respond to medication, botulinum toxin injection maybe offered. Botulinum toxin paralyzes or weakens the dystonic muscle and may be able to bring it down to near normal activity. It can be used for excessive blinking, jaw opening, neck turning, and involuntary muscles of the limbs and back.
In the later stages, when medication and botulinum toxin injection become less effective, surgery maybe offered. Studies have shown that the most effective form of surgery is deep brain stimulation (DBS). On average, it reduces symptoms by about 70%, and possibly higher reduction in some individuals.
Because DBS is an both an extensive and expensive surgery, other possible surgeries that do not use implants may be considered. Both pallidotomy surgery and MR-guided focused ultrasound will reduce symptoms by about 40%. Because these surgeries are done one side at a time, improvement may only be mostly on one side until the other side of the brain is addressed.
Research and Advocacy
Advocacy Groups
🌐 Movement Disorders Society of the Philippines
Patient Support Groups
🌐 XDP Dystonia Philippines (Facebook)
🌐 X-traordinary Women of XDP